

Introduction: Allogeneic hematopoietic stem cell transplant (allo-HCT) is a potential curative therapy for a variety of both malignant and nonmalignant hematologic disorders. However, allo-HCT is costly and requires highly specialized, technologically advanced care that is only available in select healthcare centers across the country. Due to its cost and limited availability, minority populations are at risk for healthcare disparities in access to and outcomes of allo-HCT. Prior studies have focused on the impact of health disparities, including race, and geographic residence at time of transplant, on allo-HCT outcomes with variable results. The aim of this study was to evaluate the impact of race and location of residence on outcomes of allo-HCT at one major referral institution.
Methods: We performed a retrospective cohort study of patients that underwent allo-HCT at the Ohio State University from 1984 to 2018. The impact of demographic factors including race and place of primary residence were assessed. Patients were divided into race defined as Caucasian, African American (AA), and other. They were also grouped by zip code into rural, suburban, and urban groups. Rural was defined as less than 1000 people per square mile, suburban between 1000-3000 people per square mile, and urban greater than 3000 people per square mile. 2018 population estimates were used. Patients were then stratified into 7 groups based on year (yr) of transplant for analysis. Group (gp) 1 included 1984-1988, gp 2 1989-1993, gp 3 1994-1998, gp 4 1999-2003, gp 5 2004-2008, gp 6 2009-2013, and gp 7 2014-2018. Primary endpoints were progression free survival (PFS) and overall survival (OS). PFS and OS were calculated using Kaplan Meier Curves and compared using log-rank test between race and residence groups.
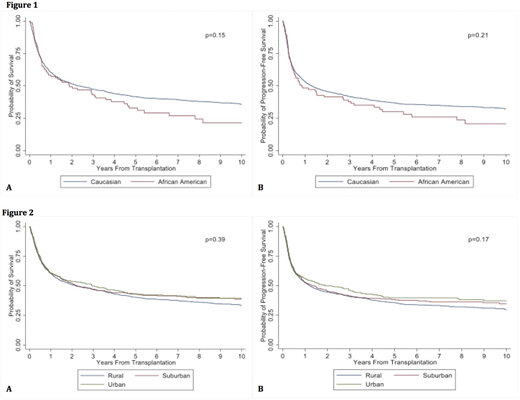
Results: A total of 1,943 patients were included in the study. Of these patients, median age at time of transplant was 50 years old (range 18-76), and 59.6% were male. AML/MDS patients made up the majority of the cohort at 46.3%, with the other most common diagnoses being non-Hodgkin's lymphoma (14.2%), acute lymphocytic leukemia (11.8%), and chronic myeloid leukemia (10.1%). Most patients (94.3%) identified as Caucasian, while 4.6% identified as AA, and 1.1% other. The majority of patients lived in a rural area at the time of transplant with 63.4% rural, 22.9% suburban, and 13.8% urban. There was no significant difference in OS or PFS between Caucasian and AA patients (Figure 1A and B; p=0.15, 0.21). Median OS for AA was 1.9 yrs [95% confidence interval (CI): 0.8-3.6] as compared to 2.3 yrs (95% CI: 1.9-2.9) for Caucasians, with 5 -yr OS of 33 vs. 42% and 10-yr OS of 21 vs. 36% for AA and Caucasian, respectively. Median PFS was 0.9 (95% CI: 0.5-2.7) and 1.3 yrs (95% CI 1.1-1.6), with 5 -yr PFS of 30 vs. 37% and 10-yr PFS of 21 vs. 32% for AA and Caucasian, respectively. There also was no significant difference in OS or PFS between rural, urban, and suburban patients (Figure 2A and 2B; p=0.39, 0.17), with median OS in the three groups 2.2 (95%CI: 1.7-2.9), 2.9 (95%CI: 1.6-4.5), and 2.2 (95% CI: 1.6-3.6) yrs, and 5-yr OS of 40 vs. 43 vs. 43% and 10-yr OS of 33 vs. 39 vs. 39%, respectively. Median PFS were 2.2 (95%CI: 1.7-2.9), 2.9 (95%CI: 1.6-4.5), and 2.2 yrs [95% CI: 1.6-3.6], with 5-yr PFS of 36 vs. 40 vs. 38% and 10-yr PFS of 30 vs. 37 vs. 35%, respectively.
Conclusion: Our study suggests that once patients undergo allo-HCT, there is no significant difference in outcomes between patients based on race or residence. This finding suggests that while these underserved populations may initially have less access to specialized care for HCT, if they ultimately undergo allo-HCT, outcomes are similar to their counterparts. Our study did show a significantly lower rates of allo-HCT performed in non-Caucasian races (94% Caucasians vs 4.6% AA and 1% other), which may reflect disparities in access to care in these groups as well as a lack of donors. Further research is needed to assess the barriers for these underserved patients to undergo transplant and to help ameliorate these barriers.
Chaudhry:Sanofi: Consultancy, Membership on an entity's Board of Directors or advisory committees. Bumma:Amgen: Speakers Bureau; Sanofi: Speakers Bureau. Khan:Amgen: Consultancy; Janssen: Consultancy. Devarakonda:Janssen: Consultancy. Vasu:Janssen: Membership on an entity's Board of Directors or advisory committees; Omeros: Membership on an entity's Board of Directors or advisory committees; Kiadis Inc: Other: Kiadis has obtained exclusive licensing requirements from The OHio State University. Jaglowski:Kite, a Gilead Company: Consultancy, Research Funding; Juno: Consultancy; Novartis: Consultancy, Research Funding; CRISPR: Consultancy. William:Merck: Research Funding; Celgene: Consultancy, Honoraria; Dova: Research Funding; Seattle Genetics: Research Funding; Incyte: Research Funding; Guidepoint Global: Consultancy; Kyowa Kirin: Consultancy, Honoraria. Mims:Syndax Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees; Kura Oncology: Membership on an entity's Board of Directors or advisory committees; Leukemia and Lymphoma Society: Other: Senior Medical Director for Beat AML Study; Agios: Consultancy; Novartis: Speakers Bureau; Jazz Pharmaceuticals: Other: Data Safety Monitoring Board. Brammer:Seattle Genetics, Inc.: Speakers Bureau; Celgene Corporation: Research Funding. Efebera:Celgene: Research Funding; Pharmacyclics: Research Funding; Takeda: Honoraria, Speakers Bureau; Ohio State University: Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal